Plantarfascitis
What is the Plantar fascia ?
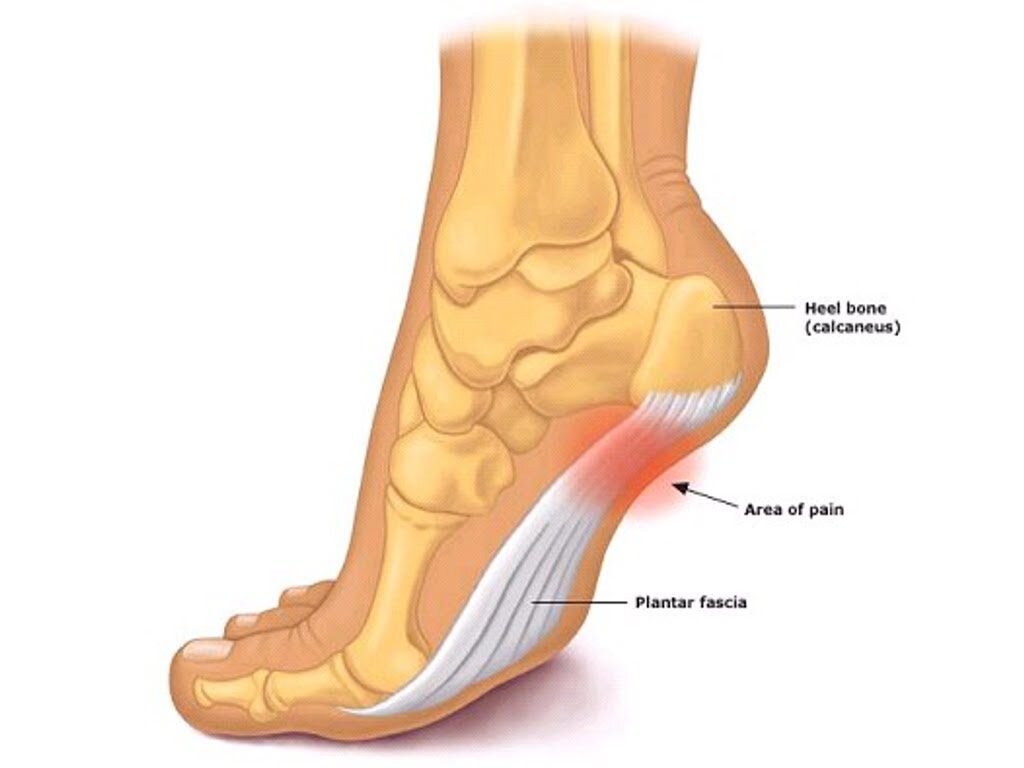
The Plantar fascia is a thick band of tissue made up of collagen fibres which is located under the foot. It runs from the heel towards the toes and its main roles are to support the arch of the foot and to assist in propelling us forward. Due to its location it takes a substantial amount of strain which can lead to the development of micro tears. These tears are a sign that the fascia is acutely inflamed- you experience this pain at the heel or in the arch of the foot.
What is the difference between Plantar fasciopathy, fasciits and fasciosis?
Plantar fasciopathy is the umbrella term for pain experienced in the heel of the foot, due to the plantar facia taking excessive load. This is similar to tendon injuries whereby its about load management and load capacity issues.
Plantar fasciitis is the inflammation of the plantar fascia. The term ‘itis’ in medicine means inflammation.
Plantar fasciosis refers to a phase in the condition when the tissue breaks down. Plantar fasciitis occurs in the initial stage of plantar fasciopathy,
I’m confused- why is it important to know the difference between the above terms?
The term Plantar fasciitis is commonly used in the literature when it is actually referring to the degeneration of the tissues instead of the actue inflammatory stage. This misdiagnosis could then lead one to utilise acute management strategies (such as ice, anti-inflammatories and rest) instead of more appropriate exercises and treatment which focus on the cause of the pain. More accurate terminology (yes- it can still be confusing!) helps us to understand the source of the pain and come up with the most appropriate treatment in order to restore function.
Who does Plantar fasciopathy affect?
Risk factors include:
• Obesity: an increased BMI is associated with up to 70% of cases
• Runners and people who spend a lot of time on their feet: may account for 8% of all running related injuries
• Loss of big toe extension
• Loss of ankle range of movement
• Reduced achillies/ calf flexibility
• Flat feet
• A sudden change or increase in physical activity: symptom onset occurs when the plantar fascia is unable to cope the this increased demand placed upon it.
Symptoms of Plantar fasciopathy
• Pain and stiffness at the base (bottom) of the heel towards the inside of the foot
• Pain is worse in the morning with the first few steps (often described as walking on glass)
• Pain is worse after rest or prolonged activity
Stage 1: Plantar fasciitis
• Can last between 6-8 weeks
• Dominated by pain
• The morning ‘hobble’ and reduced ability to perform daily activities/ sports.
Stage 2:
• Can start to gradually load the fascia with specific strengthening exercises (see protocol and image below)
• Usually non painful
• Can continue for 18 months
What is the Treatment?
Stage 1: Rest from aggravating activities, gel inserts to reduce load, anti- inflammatories, ice therapy
Stage 2: High Load strength training (Ratleff., et al, 2015) which comprises of single leg heel raises with a towel under the toes (which increases the load placed on the plantar fascia) performed every second day.
Protocol:
• Raise up onto the toes for 3 seconds, hold at the top for 2 seconds and take 3 seconds to lower. (See image below)
• Start at 12 reps x 3 sets
• After 2 weeks increase load (using a rucksack with books) perform10 reps x 4 sets
• After 4 weeks perform 8 reps x 5 sets (add more weight to backpack as you get stronger)

Ratleff et al found that high load strength training (as described above) and shoe inserts produced superior results compared to plantar fascia stretching and shoe inserts. It must be emphasised that the calf raises must be completed slowly under control to reduce the risk of symptoms flaring.
Why do the strengthening exercises help?
There is still a limited understanding about why this high-load strength training may work in the treatment of plantar fasciopathy. One theory could be that strength training may stimulate increased collagen synthesis (production of collagen), which helps to return the tendon its normal state, as well as increasing the ability of the plantar fascia to take load, thus improving functional outcome.
The second theory is that the strength training may help improve the ankle strength and range of movement (mainly dorsi flexion) as well as the strength of the deep foot muscles.
Take Home Message
Perform the high load strengthening exercises slowly!
References
https://blogs.bmj.com/bjsm/2014/09/15/plantar-fasciitis-important-new-research-by-michael-rathleff/
https://enertor.com/blogs/enertors/plantar-fasciitis-vs-plantar-fasciopathy
Kongsgaard M, Kovanen V, Aagaard P, et al. Corticosteroid injections, eccentric decline squat training and heavy slow resistance training in patellar tendinopathy. Scand J Med Sci Sports 2009;19(6):790-802 doi: 10.1111/j.1600-0838.2009.00949.x[published Online First: Epub Date]|.
https://www.nhs.uk/conditions/plantar-fasciitis/
Rathleff MS, Mølgaard CM, Fredberg U, et al. High-load strength training improves outcome in patients with plantar fasciitis: A randomized controlled trial with 12-month follow-up. Scand J Med Sci Spor 2014:n/a-n/a doi: 10.1111/sms.12313[published Online First: Epub Date]|
Stecco C, Corradin M, Macchi V, et al. Plantar fascia anatomy and its relationship with Achilles tendon and paratenon. Journal of anatomy 2013;223(6):665-76 doi: 10.1111/joa.12111[published Online First: Epub Date]|.